Mirels score calculator: Pathological fracture risk in long bone metastasis
The Mirels score is used to assess the risk of pathological fracture in patients with a long bone metastasis. Originally published in 1989 the score uses three radiographic and one clinical variable to assess risk (1).
Fracture risk is divided into one of three categories:
Evidence
The score is based on a retrospective analysis of 78 metastatic bone lesions that had been irradiated without prophylactic fixation. The study found that over a 6-month period 51 lesions did not fracture and 27 lesions fractured. The mean Mirels score was 7 in the non-fracture group and 10 in the fracture group. The combined score was found to have the highest accuracy in predicting fracture risk on receiver operator characteristic (ROC) curve analysis as compared to any individual predictor variable alone. The overall sensitivity and specificity of the Mirels score is estimated to be 91% and 35% respectively(2).
Limitations of the Mirels score are that the relatively low specificity can potentially result in unnecessary fixations. There are also concerns about reproducibility as some variables such as size of lesion and nature of lesion can be subjective(3). Also lesion site is included as a predictor variable but in the original study this variable was not significantly associated with fracture risk. The number of samples in the study were small and could not determine if particular primary tumour types are more significantly associated with fracture risk.
Despite these limitations, the Mirels score remains a valid and widely used tool to assess risk of pathological fracture. It has been independently validated(4,5) and was considered a useful aid in the British Orthopaedic Oncology Society guidelines(6).
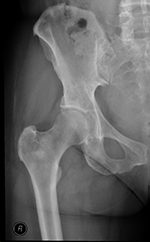
Radiographic examples
References:
- Mirels H. Metastatic disease in long bones. A proposed scoring system for diagnosing impending pathologic fractures. Clin Orthop Relat Res. 1989;(249):256-264.
- Jawad MU, Scully SP. In brief: classifications in brief: Mirels’ classification: metastatic disease in long bones and impending pathologic fracture. Clin Orthop Relat Res. 2010;468(10):2825-2827. doi:10.1007/s11999-010-1326-4
- Howard EL, Shepherd KL, Cribb G, Cool P. The validity of the Mirels score for predicting impending pathological fractures of the lower limb. Bone Joint J. 2018;100-B(8):1100-1105. doi:10.1302/0301-620X.100B8.BJJ-2018-0300.R1
- Evans AR, Bottros J, Grant W, Chen BY, Damron TA. Mirels’ rating for humerus lesions is both reproducible and valid. Clin Orthop Relat Res. 2008;466(6):1279-1284. doi:10.1007/s11999-008-0200-0
- Damron TA, Morgan H, Prakash D, Grant W, Aronowitz J, Heiner J. Critical evaluation of Mirels’ rating system for impending pathologic fractures. Clin Orthop Relat Res. 2003;(415 Suppl):S201-7. doi:10.1097/01.blo.0000093842.72468.73
- British Orthopaedic Oncology Society Guidelines. Published online 2015. http://www.boos.org.uk/wp-content/uploads/2016/03/BOOS-MBD-2016-BOA.pdf